Blog
Ultrasonic Scaling: Aerosol or Drip from the Tip? What Does the Evidence Say?
Expert Advice for Implementing Aerosol Management at Your Practice
Nancy Miller, RDH, recalls not wearing masks or gloves in the days before HIV emerged as a deadly pathogen. Just as HIV brought attention to bloodborne pathogens, COVID-19 has aimed a spotlight on airborne pathogens in the dental office. Dental aerosols are primarily created by high-speed handpieces and ultrasonic scalers, air/water syringe tips, and air abrasion devices. Fortunately, says Miller, “We’re already experts on infection control, and we can take practical steps to protect ourselves, our co-workers, and our patients against this new airborne threat.”
Expert Guidance
OSHA considers dental workers in a “very high exposure risk” category for SARS-CoV-2, the virus that causes COVID-19.1 Official guidance from the Centers for Disease Control and Prevention (CDC) prioritizes using hand instrumentation over ultrasonic instrumentation and instituting methods for aerosol reduction (Table 1). Ultimately the use of ultrasonic instrumentation is based on procedure and the best clinical judgment of the operator. Anecdotal evidence shows some hygienists prefer not to abandon ultrasonic scaling but need assurance that disease transmission is minimized and that they and their patients are safely protected from splatter/droplets/aerosols and the viruses and bacteria contained within.
Table 1. Recommended Aerosol Reduction Methods
Should aerosol generating equipment such as dental handpieces, air/water syringes, or ultrasonic scalers be used, HuFriedyGroup recommends adherence to the aerosol reduction methods outlined by the Centers for Disease Control and Prevention.2
- Use four-handed dentistry, high evacuation suction, and dental dams to minimize droplet spatter and aerosols.
- Limit the number of personnel present during the procedure to only those essential for patient care and procedure support.
- Have patients use preprocedural mouth rinses (PPMR). The American Dental Association’s Interim Guidance for Minimizing Risk of COVID-19 Transmission recommends that patients rinse with 1.5% hydrogen peroxide or 0.2% povidone before each appointment.
Using Ultrasonic Scaling in the Dental Office
 Miller has returned to her practice by adapting familiar procedures to protect herself, her co-workers and her patients. She notes that “aerosol management” may be the new buzz word, but says it was always critical. Research shows that up to 90% of ultrasonic aerosols can be eliminated via the use of high-volume evacuation (HVE) during ultrasonic scaling procedures.3 The key is to achieve safety by building up layers of protection, starting with appropriate personal protective equipment (PPE), and focusing on controlling aerosols as close to the patient’s mouth as possible. This may mean changing procedures that have become second nature.
Miller has returned to her practice by adapting familiar procedures to protect herself, her co-workers and her patients. She notes that “aerosol management” may be the new buzz word, but says it was always critical. Research shows that up to 90% of ultrasonic aerosols can be eliminated via the use of high-volume evacuation (HVE) during ultrasonic scaling procedures.3 The key is to achieve safety by building up layers of protection, starting with appropriate personal protective equipment (PPE), and focusing on controlling aerosols as close to the patient’s mouth as possible. This may mean changing procedures that have become second nature.
For example, surveys and clinical observations show that clinicians tend to attach the insert or tip to the ultrasonic handpiece, adjust power and water levels until a robust aerosol is generated, and proceed to power scale. The water aerosolization and the high-pitched sound emitted are taken as signals that the insert/tip is ready for use, but that assumption is incorrect and not supported by the scientific evidence.
What Does the Evidence Say?
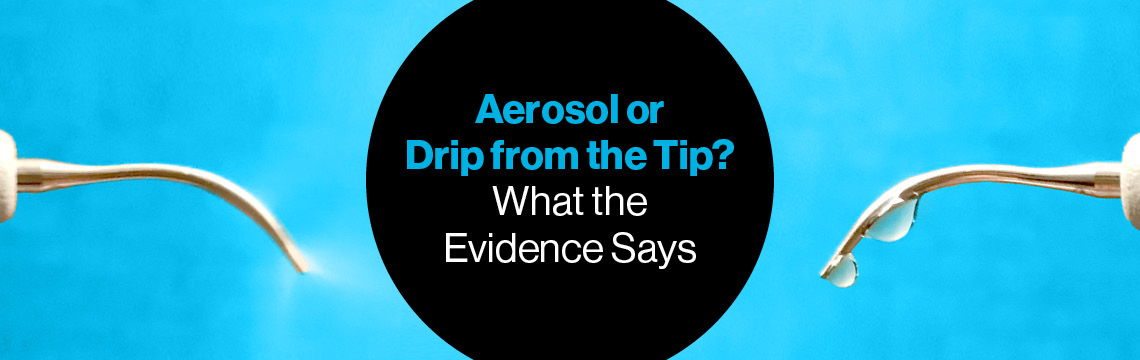
The goal of water flow in ultrasonic scaling is not aerosolization but rather enough water flow to cool the tip and prevent overheating – approximately 20 ml/minute (about four-and-a-half teaspoons). Low to medium power settings generally create streaming and/or drips from the tip. Medium to high power settings generally aerosolize the water, as the higher amplitude causes water droplets to atomize. Atomized water does not reach the working end of the tip, so heat regulation of the tip does not occur at these higher settings.
Instead, the evidence-based recommendation for water flow is: “a flow rate that effectively cools and maximizes cavitation and microstreaming activity is one that produces intermittent droplets at the activated tip…The recommendation to produce droplets at the tip is evidence-based and in contrast to instrumentation guidelines suggesting the production of a fine mist or halo at the tip.”4
What About Ultrasonic Scaling Performance?
So, will using a drip instead of an aerosol result in effective ultrasonic scaling? Yes, says Miller. “The lower power creates less aerosol and actually cools the tip more effectively. It may take a bit of getting used to not using an aerosol, but evidence supports the use of a rapid, intermittent drip.”
With rapid intermittent drips, water flows over the tip and reaches its end, advancing cavitation and microstreaming activity in periodontal pockets. Contrast that with streaming water flow, where excess water flows over the tip in a stream that can produce a dampening effect on the tip movement – the more water the more dampening. Finally, with aerosolization, energy is expended on creating the aerosol rather than on supporting tip movement.5
How Do I Implement Aerosol Management?
For Miller aerosol containment begins in the patient’s mouth and minimizes aerosol generation. Hygienists have the opportunity to minimize aerosols in the first place. That means using appropriate power levels for inserts/tips. Power level recommendations are printed on packaging included with the insert/tip. Generally, the thinner the tip the lower the power that should be used. Adjust the power level for each insert/tip, then adjust the water until a rapid flow of droplets is released from the tip.
Additional layers of protection can help make the dental environment safer. “Adding a pre-rinse reduces the oral flora that can become airborne during dental procedures and reassures the patient that you’re doing what’s best for them,” says Miller. Inside the mouth a saliva ejector removes liquid from the back of the mouth where it collects, but is too small to capture sprays. “For that you need HVE and a larger tip, at least eight millimeters, placed close to the treatment site. This is especially important at the front of the mouth where aerosols can easily escape.” She adds that using HVE is easiest with four-handed dentistry, yet most hygienists do not have assistants. A shorter HVE tube and lighter weight hose adapter will simplify solo work. Learning to juggle more equipment requires patience and not giving up while you’re learning. “Remember that with these new practices you’re protecting yourself, your patient, and the next patient who will be in your chair.”
References
1 Occupational Safety and Health Administration (OSHA), Department of Labor. Guidance on preparing workplaces for COVID-19 (OSHA 3990-02 2020). Available at: www.osha.gov/Publications/OSHA3990.pdf.
2 Centers for Disease Control and Prevention (CDC). Framework for healthcare systems providing non-COVID-19 clinical care during the COVID-19 pandemic. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/framework-non-COVID-care.html.
3 Harrel SK, Molinari J. Aerosols and splatter in dentistry, JADA 2004;135:429-437.
4 George M, Donley T, Preshaw P. Ultrasonic Debridement, Theory and Technique. John Wiley and Sons; 2014: 52-55.
5 Lea SC, Landini G, Walmsley AD. Vibration Characteristics of ultrasonic scalers assesses with scanning laser vibrometry. J Dent 2002; 30: 147-51
All company and product names are trademarks of Hu-Friedy Mfg. Co., LLC, or Crosstex International, Inc., its affiliates or related companies, unless otherwise noted.